
Cart
0
$0.00


If you would like to understand the risks and benefits of vaginal breech birth vs. cesarean section, we suggest that you watch this presentation.
This 80-minute lecture covers the evidence on term singleton breech outcomes over the past 2 decades. You will learn about short- and long-term risks to the baby, short- and long-term risks to the mother, and the risks to the mother's future pregnancies.

This 1-hour lecture covers the evidence on outcomes of community breech birth (home or birth center). Looking at all studies that mention community breech outcomes over the past 20 years, Dr. Rixa Freeze discusses the strengths and weaknesses of each study.

This 71-minute lecture gives a detailed look at the risks and outcomes of different types of breeches (frank, complete, footling, etc.). It also discusses how breeches are classified and why we should adopt a universal, consistent nomenclature system.
Vaginal Breech Birth: Why It's Important and How It Works
(free lectures)

This lecture, sponsored by Project ECHO and the University of Utah, covers why training in vaginal breech birth is important and how normal vaginal breech birth works, from the emergence of the baby's buttocks until the birth of the head. Register here!

Questa lezione, sponsorizzata dal Progetto ECHO e dall'Università dello Utah, spiega perché è importante la formazione sul parto vaginale podalico e come funziona il parto vaginale podalico normale, dalla comparsa dei glutei del bambino fino alla nascita della testa. Iscriviti qui!
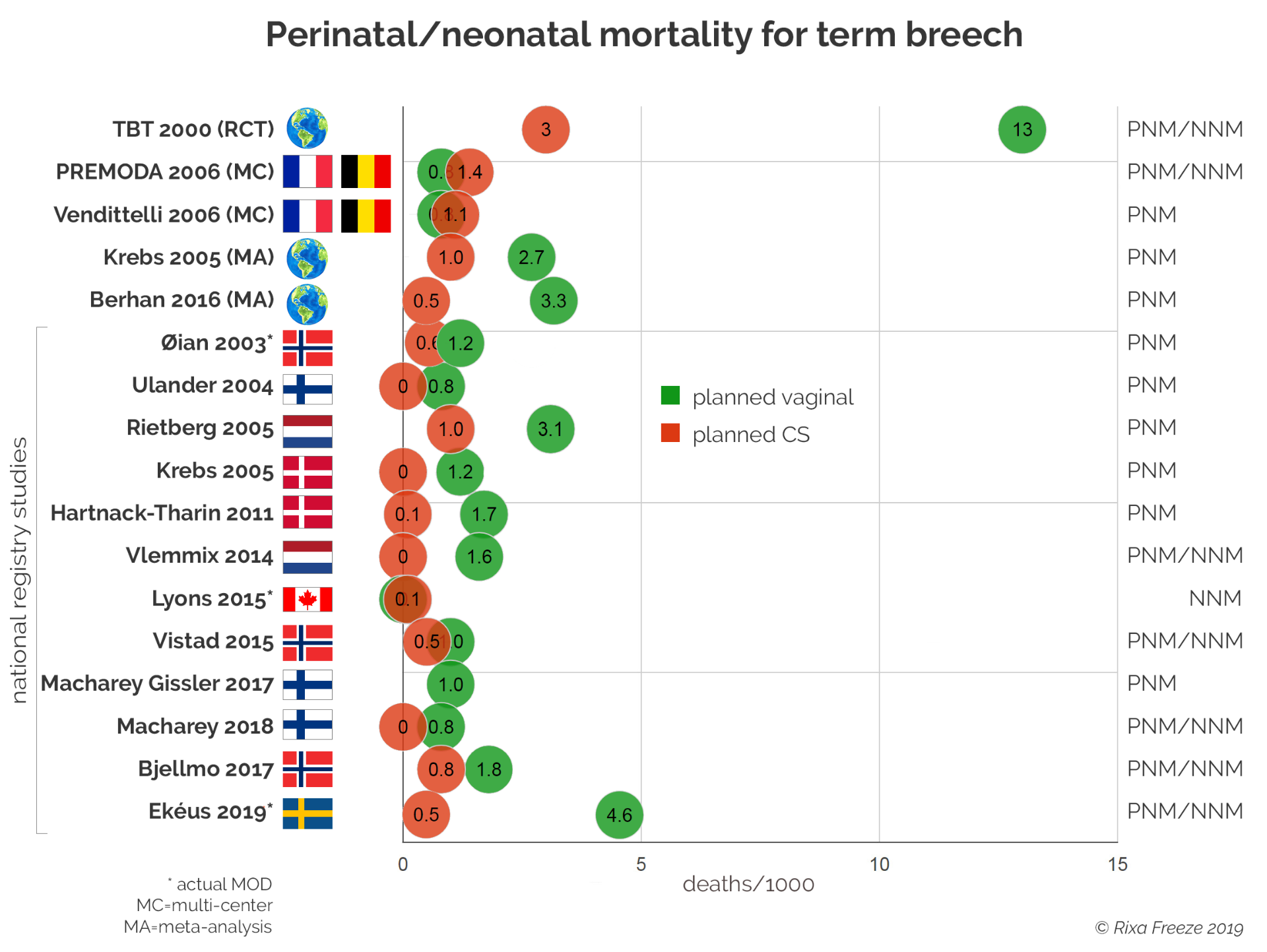
Recent studies do not support the findings of the 2000 Term Breech Trial, a randomized controlled trial that enrolled 2,088 women.
Two large multi-center studies in France and Belgium found no difference in perinatal/neonatal mortality between planned CS and planned vaginal birth. These studies--one prospective, one retrospective--followed over 10,000 women and had 174 & 175 participating hospitals.
Some national registry studies have found no significant differences between planned CS and planned vaginal breech birth.
A meta-analysis and other registry studies have found some short-term advantage to planned CS, but the advantage is significantly less pronounced than in the Term Breech Trial.
Rixa Freeze, PhD

Making a decision about how to birth a breech baby involves a complex risk calculus. Women have to weigh the short- and long-term benefits to themselves, their babies, and their future pregnancies. This graphic shows how planned CS for breech has affected women and their babies in the Netherlands.
A study by Verhoeven et al (2005) discusses the effects of the increase in planned CS since the Term Breech Trial. The results show a risk trade-off.
"Between 2001-2005, 8,500 women in the Netherlands had a planned CS for breech. This increase in pCS saved an estimated 19 babies, but it also led to 4 direct maternal deaths, 9 additional babies dying in future pregnancies due to the uterine scar, and 140 additional life-threatening maternal complications in future pregnancies."
Rixa Freeze, PhD

The Number Needed to Treat (NNT) is a simple calculation showing how many treatments are needed to prevent one bad outcome. The lower the NNT, the stronger the benefit of the treatment.
For example, a NNT of 5 means that you only need to perform 5 treatments to prevent one bad outcome. That is a very strong NNT. A NNT of 500 means that you need to perform 500 treatments to prevent one bad outcome, showing that the treatment has a very weak effect.
With breech, the most pertinent question is: how many cesareans are needed to prevent one baby from dying?
The Term Breech Trial found a NNT of 104, meaning that one baby was saved for every 104 c-sections. However, that number was only true in the short term. A long-term followup study found that there was no difference in rates of death or neurodevelopmental delay at 2 years of age. In other words, routine cesarean section for term breech had no long-term advantages.
More recent studies have found much higher NNTs than the Term Breech Trial, ranging from 175 to 666. And some studies, such as PREMODA (Goffinet 2006), have found no differences in perinatal mortality or morbidity between vaginal breech birth and planned CS. In this study, there is no NNT.
Rixa Freeze, PhD

A Dutch registry study by Vlemmix et al (2014) calculated what would happen if all of the Dutch women who still choose vaginal breech birth were to have planned cesarean sections. The researchers estimated that it would take 649 planned c-sections to prevent 1 neonatal death, 2 birth traumas, and 11.6 low Apgar scores.
However, cesarean sections also come with risks: to the baby, to the mother, and to the mother's future pregnancies. For every baby saved in this scenario, 648 women will have had unnecessary surgery and will face additional risks due to the c-sections for the rest of their lives.
Rixa Freeze, PhD